

1.6k words, 7 min read
Editor’s note: This is the last of 5 essays in The Cycle, my series and concept for my upcoming book on healthcare’s revenue cycle. Previous writing here.
At twenty-five, I thought I’d made it. Charcoal suit, Tumi bag, flying out of NYC on someone else’s dime, racking up hotel points for a job at Deloitte — one of the faceless Big Four consulting firms — as a type-A asshole with a client laptop and a per diem. So when that same job flew me to Cedar Rapids, Iowa, and dropped me in an office park owned by the local hospital to solve problems like how to fax an insurance company faster, I decided, naturally, that the work was beneath me.
One project actually sat me at a hospital registration desk, checking patients in during an Epic Prelude cutover to prove the system worked. It mostly proved the opposite. The field for the group number took only digits, but half the cards had letters. The fields didn’t line up with the boxes on my screen. And a line built up behind a woman about my mother’s age, a folder of her own paperwork in her lap, who’d booked weeks ago and only wanted to be seen - while I, the suit who only knew how to make PowerPoint slides, sat there unable to check her in.
The disdain came with the job. Consulting (whatever that means) works in rotations - a few months on one project, a few on the next, until you pick a lane and stay. The prestige lanes were strategy (whatever that means), or M&A, or if you were lucky a confidential engagement with a mysterious James Bond code name like Project Goldfinch. Revenue cycle — the billing office, the part of a hospital that turns care into money — was where you rotated when you hadn’t earned anything better. Up close, it’s faxing, calling, and chasing claims through insurance portals. Kids like me were in it for the airline miles and the story to tell at dinner, angling for the deal team or a pitch with a billion-dollar market on slide three. I rotated through it like everyone else. I just didn’t know how many times I’d rotate back.
And it isn’t just consultants. Almost everyone in healthcare has trained themselves to look down on the revenue cycle. The founders raising money to “fix healthcare” figure it just takes their big brains to drag the billing office out of the stone age - plumbing for a place they assume has no running water. One healthtech CEO called it “the transactional bowels of U.S. healthcare“. There’s a running joke in the industry that every AI scribe company becomes an RCM company anyway, as if settling for the money grab.
The doctors and nurses treat it as the bureaucracy between them and the patient - the reason they’re on the phone at night instead of at the bedside. And the reformers have their favorite villain — administrators — and a misleading chart, the one that makes the rounds every few months: the reformers’ favorite chart while the number of doctors barely moves. The point is always the same: too much bureaucracy, too much overhead, too many people pushing paper instead of caring for patients.
If you work in rev cycle management (RCM), you already know all this. Tell someone at a party what you do and they don’t change the subject - they start telling you about the afternoon they lost on hold, transferred four times to fix a bill that was wrong in the first place. They’re not wrong that it’s a mess. They’re wrong about what the mess is.
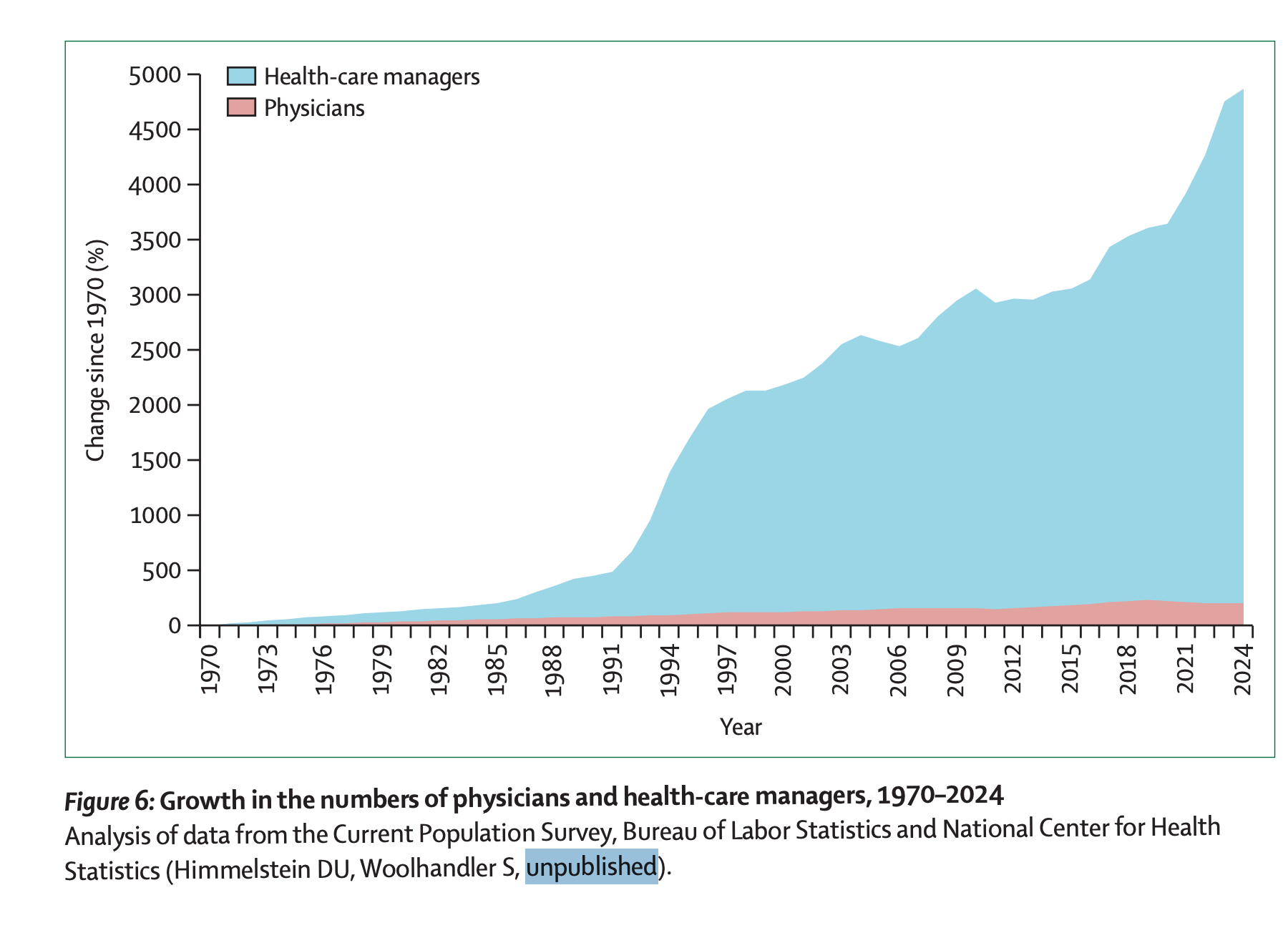
The chart gets one thing right - it’s enormous. Well over a million people in this country work as medical secretaries and administrative assistants — just one clerical slice of the revenue cycle — more than the roughly 870,000 doctors who actually see patients. Depending on who’s counting, somewhere between a sixth and a third of every dollar in American healthcare goes to administration rather than care. Nearly three out of four insured adults do some kind of paperwork or phone-chasing for their own care every year, and about a quarter of them put off seeing a doctor to avoid it.
So it isn’t a small thing. It might be the biggest thing. Which raises a question I spent years not asking: why does everyone - me included - look down on it?
The simplistic answer is greed. Administrators multiplying to justify their own salaries, vendors selling hospitals software they never asked for, a whole industry billing for the privilege of getting a hospital paid. And it isn’t wrong, exactly - there is waste, there are rent-seekers, there are people getting rich off the confusion.
But greed doesn’t explain the scale, or the tangle. It doesn’t explain why moving healthcare’s money grew so complicated, so confusing, and so consequential to the care itself that you can’t do anything in this industry without inevitably getting caught in the cycle.
What makes it so tangled is that underneath, it’s a philosophical problem.
Every hospital bill is a clumsy answer to an unspoken and unsolvable question: what is a human life worth in dollars? Who deserves a cure they can’t pay for? What do we owe a stranger who’s sick?
Philosophers, priests, and politicians have argued those for centuries and never settled them. Healthcare doesn’t get to wait for the argument to end. The patient is here now, and the cure is in reach—a sickle-cell therapy that took decades of science and manufacturing to invent—for over two million dollars. Someone has to decide - today - whether she gets it and who pays. So American healthcare answers the unanswerable by default, millions of times a day, in a language of codes and denials and adjustments - sterilized until it bears no resemblance to a moral choice at all.
It’s right there in the vocabulary. The share of the bill left to the patient is called their responsibility - as if owing for your own illness were a question of character.
And the question doesn’t vanish under a different system; it actually gets put out in the open. In Britain, a public board called NICE decides what a year of healthy life is worth - for years £20,000 to £30,000, recently raised - and turns down treatments priced above the line. America would rather every insurer set their own policy and answer it one denial at a time.
Strip away the codes and the call centers, and that’s the work underneath. Revenue cycle is where American healthcare turns a moral question into a financial answer. So if it’s a moral question, why do we only ever try to make the answer cheaper?
For as long as I’ve been around it, every attempt to fix the revenue cycle has been to make it cheaper. Health systems outsource the work to a call center outside of Memphis, then to the Philippines. Automate the easy claims and write off the small ones. Work the accounts that pay and drop the ones that don’t. Spend less money on collecting money.
Funnily enough, there’s always more of this work, not less. Decades of outsourcing and automation, and denial rates have only climbed - with more than half of providers saying it’s getting worse, not better. Every efficiency is short-lived, because the rules change beneath it every year - a new payer policy, a new code set, a new reason to deny. We keep trying to make the RCM machine more efficient, when the complicated part is allocating scarce healthcare resources. You can’t automate “what is this worth” when the answer swings with every election.
Five years in, Deloitte was pigeonholing me into revenue cycle, and I didn’t want it to be my whole career - so I left for something that felt like it mattered more. But every job I took next was supposed to be a step up from the billing office, and every one turned out to be another door back into it. A hospital merger that came down to whose billing system was better. A clinical trial where the hard part was getting financial approval for the science. A Medicaid plan where the work was deciding who was eligible for what. I kept trying to escape, and kept rotating back in. Everything is revenue cycle - there’s no exit in healthcare.
The relationship between medicine and the people who pay for it is the defining feature of American healthcare—not what we can do, but who we’ll do it for—and the revenue cycle is where that relationship actually happens. Nearly a third of the people who work in American healthcare never touch a patient - they work the space between the care and the money, call centers calling other call centers, and almost none of us understand how it runs.
My bet is that the market for RCM is only growing, not simplifying, despite the new promises of AI. Andreessen Horowitz, arguably the most prestigious venture firm in the country, calls this healthtech’s “biggest prize”—a multi-$100 billion industry—and every few months another startup raises a fortune promising to automate the tangle. The disdain is only skin-deep. Because underneath it, everyone is trying to own the thing that decides who gets paid, and how much.
So now I’m embracing it. I walked away from a whole career to avoid this work, and here I am writing a book about it.*
Which brings me back to that registration desk, and the woman about my mom’s age standing in line. I was annoyed she was waiting on me - and if I’m honest, part of me never stopped looking down on the work; I never learned to love it. But everything that mattered about her afternoon—whether she got seen, what it would cost her, whether she could afford to come back—was already being decided by the machine in front of me, and I was the only one at that desk who couldn’t see it. I was still trying to force the letters on her insurance card into a field that would only take numbers.
Editor’s note: This is the fifth essay in a series about the revenue cycle, which started with Not a Cycle. I published my resignation letter because I wanted the time to write a book. Ironically, I spent the early part of my career trying to get out of the revenue cycle and now I return like a prodigal son. Something poetic about the cyclical nature.
I think money and medicine is the most interesting topic, and I want to talk about healthcare claims the same way Michael Lewis talked about credit swaps in The Big Short - entertaining, and worth reading even if you don’t work in healthcare.
I’ll keep publishing revenue cycle essays now and then, and see what makes it into the book. But I write other things too - Struck by Turtle was one - and going forward you’ll see more of that from me: anthropology, history, creative deep dives (not just billing). I’m planning on tackling some hairy topics like labor disputes or religion in healthcare. The next one up will be a series about Mass General.
If you’re only here for the revenue cycle essays - or you’d rather skip them - you can set that in your subscription under The Cycle. And if you’ve got a story this machine put you through, send it my way.
Thanks for reading,
-Andrew