
Struck by Turtle, Initial Encounter
The invisible workforce translating human suffering into billable data

2.3k words, 9 min read

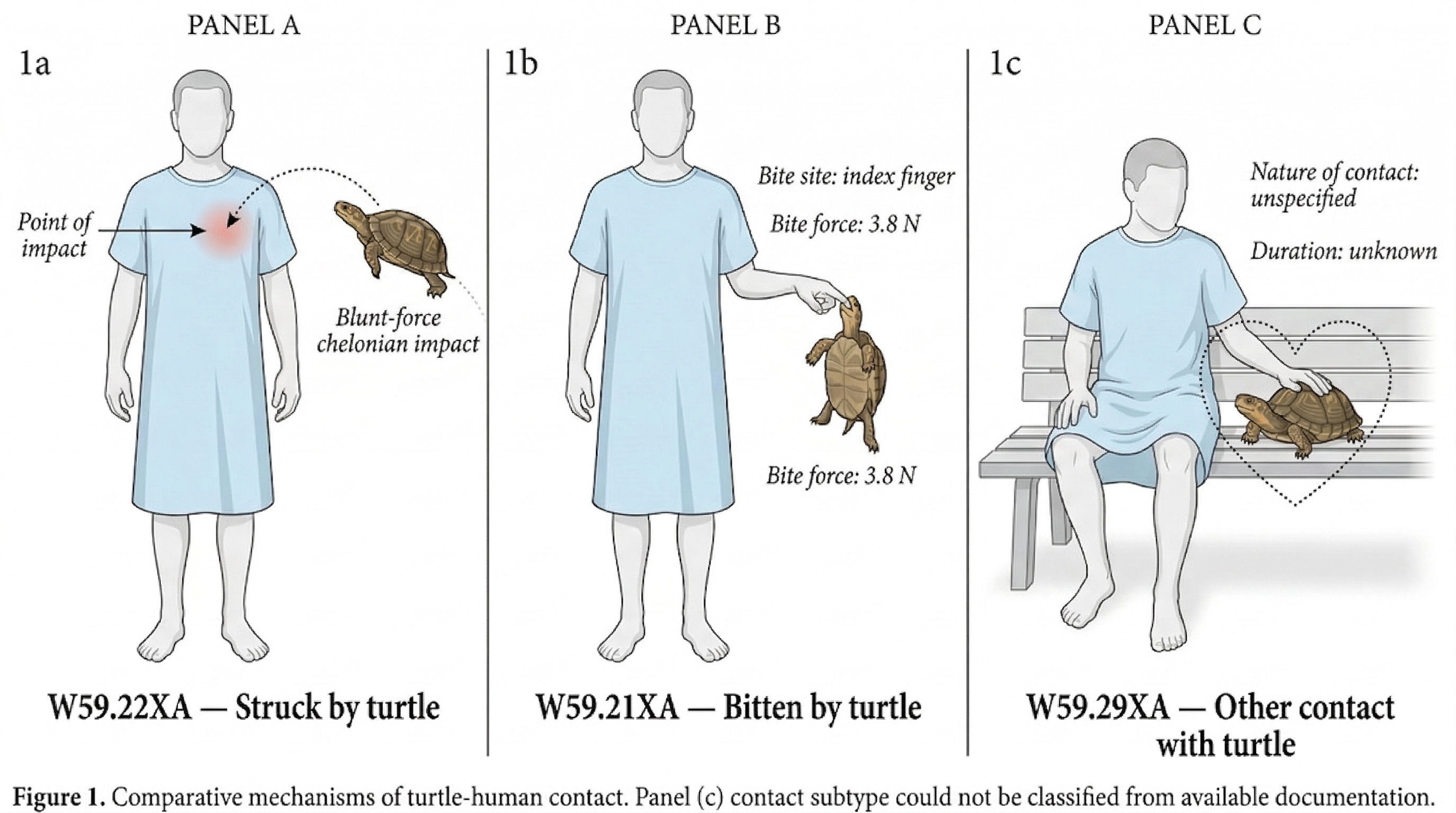
There is a medical code for being struck by a turtle — the unmemorable W59.22XA.
Every time a doctor sees a patient in America, the encounter has to be translated into a diagnosis code from the ICD-10-CM system before anyone gets paid. ICD-10 is one of several coding systems that turn a clinical encounter into a financial event. Diagnosis codes describe what’s wrong with you. Procedure codes describe what was done about it. The combination determines what the hospital collects — and the diagnosis is where it starts. Without one, nothing else in the billing chain moves. The diagnosis code for being struck by a turtle is W59.22XA. There is a separate code for being bitten by a turtle (W59.21XA), and a third for “other contact with turtle” (W59.29XA), because someone decided the distinction between being struck, bitten, and otherwise contacted by a turtle warranted three separate categories.
There is a code for burns sustained from water-skis that caught fire (V91.07XA) — not hypothetical, but a code that exists because someone showed up at a clinic with exactly this problem and the system had no way to bill for it. There is a code for “bizarre personal appearance“ (R46.1), which feels less like medicine and more like someone at the WHO took a personal grudge and made it official. And there is a code for problems with your in-laws (Z63.1) — meaning a clinician listened to a patient describe their mother-in-law, wrote it down as a medical factor, and handed it to a person whose entire job is turning that sort of thing into six characters a payment system can read. Your relationship with your mother-in-law is now a billable event.
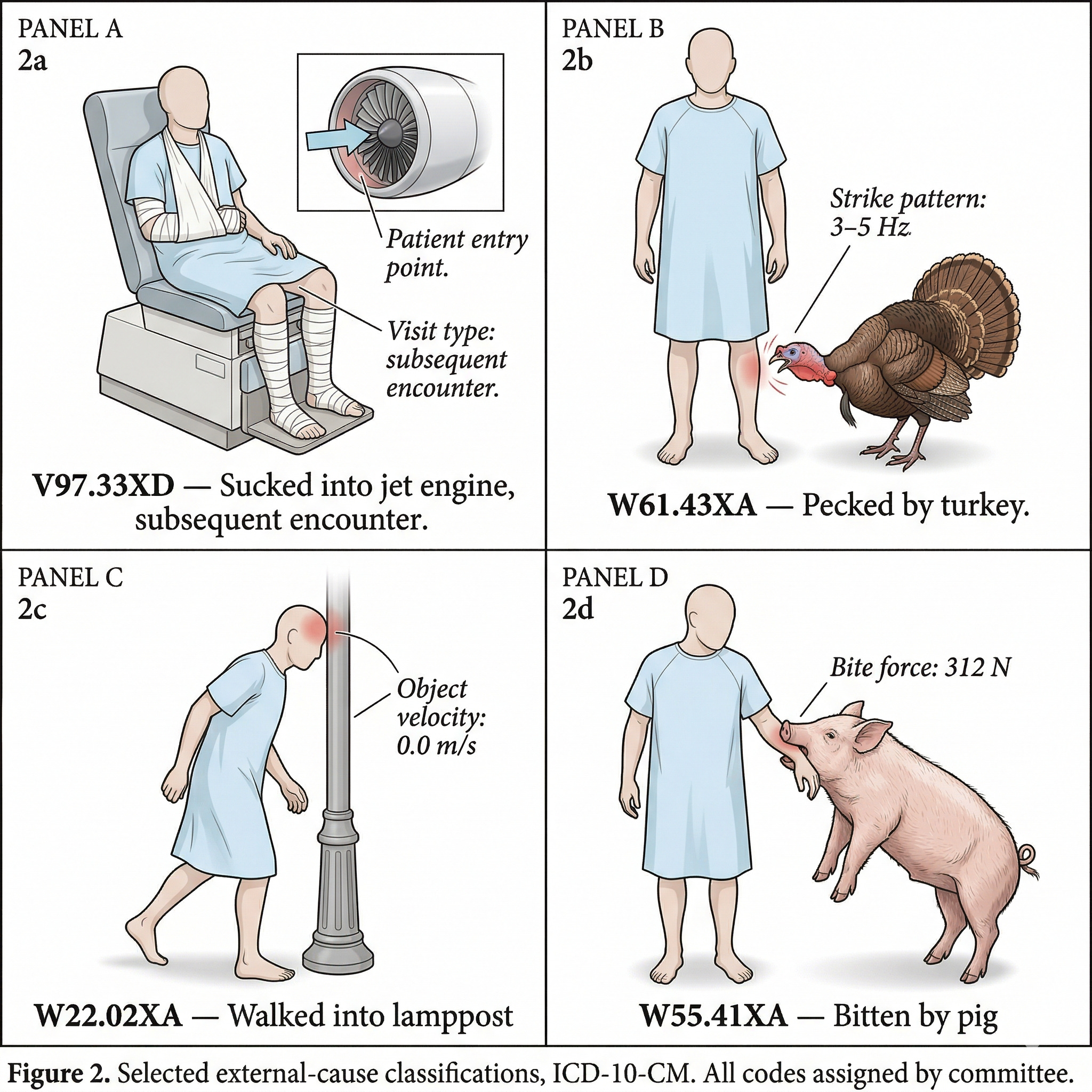
There are over 74,000 of these codes in the US system, not to mention the other 78,000 procedure codes. The WHO’s version has about 14,000 — enough to track disease and death across populations. America needed five times that. Medicare needed a language precise enough to calibrate payment, so the codes got repurposed for billing. More precision meant more reimbursement accuracy, and more accuracy meant more codes. Sucked into a jet engine, subsequent encounter (V97.33XD) — which sounds absurd until you realize “subsequent encounter” just means a follow-up visit. Someone survived a jet engine and came back. Pecked by a turkey (W61.43XA). Walked into a lamppost (W22.02XA). Bitten by a pig (W55.41XA). Actual codes, decided by humans on committees, and the committees keep meeting.
The turtle codes aren’t hurting anyone — most providers use maybe 200-300 codes regularly, and their EHR suggests the rest. There is no constituency for fewer codes and no incentive to consolidate.1 But every code requires matching documentation: physicians spend roughly 15 minutes per encounter writing notes that justify the code rather than delivering care. Medical coding is a $24B+ industry in the US alone — departments, certifications, training programs, auditing firms, all built to translate medicine into billable transactions.
The absurdity isn’t the problem. The problem is that the system needs the absurdity to function — and that need has real costs. The turtle is funny. The infrastructure behind the turtle is expensive. What happened to you, translated into what the system can pay for.
Z04.9 — Encounter for Observation for Unspecified Reason
One of my first consulting projects, at the tender age of 24, took me to a health system’s business park in Virginia. I got badged in at the lobby, rode the elevator up, and escorted through hallways lined with motivational posters — a single word in caps and a cheap phrase under a stock photo: TEAMWORK over a rowing crew, INTEGRITY over a mountain summit. We were there for a group Epic applications meeting with the department director named Chris (short for Christine). Two hours of workflow configurations in a fluorescently-lit conference room - another long workshop with fifteen people where nothing was accomplished.
On the way out of the conference room, Chris walked me through the coding department. It was a whole floor. Rows of cubicles stretching to the far wall, each one with a monitor, a stack of papers, and a woman reading through clinical charts. Copiers humming, fax machines whirring (only in a health system). A potluck in the break area — slow cooker of something, paper plates and Solo cups, a store-bought cake with frosting flowers. At the desks nearest me: a wooden “Live Laugh Love“ sign on the cubicle wall, photos of kids in football jerseys, a “Proud Army Mom“ bumper sticker on a filing cabinet. One of the ladies was trying to print something and the printer jammed. Chris stopped to help — the director wrestling with the paper tray while we stood in the aisle.
I noticed the woman at the next cubicle. She had a chart open on her screen — physician notes, lab results, a discharge summary — and she was reading it the way a lawyer reads a contract, looking for the details that changed the meaning. She paused at something in the operative note, scrolled back to compare it against the labs, then pulled up a reference window and checked two codes side by side before choosing one.
The distinction she was weighing — one complication versus two, one severity level versus the next — would change how the diagnosis and procedure codes combined, which would change the Diagnosis Related Group the case fell into, which would set whether the hospital was paid $8,000 or $13,000 for that admission. By the time Chris cleared the printer, the coder had made her call, entered the codes, and was already opening the next chart. Ten thousand dollars of clinical interpretation had just passed through her hands in the time it took to unjam a printer.
These women worked through hundreds of cases a day — reading physician notes, interpreting what happened to a patient, deciding which code fit. Each decision worth thousands to a hospital that couldn’t bill without them. I remember teaching one of them the hotkeys to cut and paste (Ctrl-C, Ctrl-V) during a break, and her reacting like I’d shown her a magic trick. Here was a woman who could read a surgical note, weigh the significance of a complication, and land on a five-figure financial outcome in fifteen minutes — and she was delighted to learn a keyboard shortcut.
The American medical coding workforce is roughly 195,000 people. Eighty-four percent are women. The typical coder is in her mid-forties, earns about $50,000 a year, and handles around fifteen inpatient cases a day — each one requiring her to build the full coded picture of the encounter, diagnosis and procedure codes together, that determines what the hospital gets paid.
That hospital — like every hospital in America — depended on that floor. Not in the way it depended on its surgeons or its ER, but in the way a business depends on accounts receivable: without it, the money stops. It is a workforce larger than the U.S. steel manufacturing industry, and one that determines how $1.6 trillion in hospital spending gets allocated, two charts at a time.
Z56.4 — Discord with boss and workmates
In a 2024 Black Book Research survey of 4,081 medical coders, 90% identified upcoding — assigning a more severe code than the documentation supports — as a major ethical dilemma. Eighteen percent reported pressure from their employer to engage in what they described as fraudulent coding for financial gain.
Physicians routinely under-document: a surgeon performs a procedure with three complications, the operative note mentions one, and the hospital gets paid for a less severe case than what actually happened. CMS’s own audits found $28.8B in improper Medicare payments in fiscal year 2025 — 6.55% of all fee-for-service claims — with incorrect coding and insufficient documentation as the leading causes. And that is Medicare alone.
For a mid-size hospital running $500M in revenue at a 3% margin, that margin is $15 million. The revenue at stake in coding accuracy — the accumulated weight of thousands of $5K-to-$15K decisions — can easily exceed it. The financial fate of the institution passes through the same hands that were unjamming the printer.
Clinical documentation integrity (CDI) programs exist to close the documentation gap — my firm had a whole practice dedicated to it. When they work honestly, the hospital gets paid fairly for care it delivered. But the skill required to close a legitimate gap is the same skill required to push past it, and 36% of CDI programs report to the revenue cycle department, not to clinical quality. The incentive to code accurately and the incentive to code profitably share the same office.
The physician sees this one way: the coding department is a black box that turns clinical work into billing outcomes she can’t fully control. She went to medical school to practice medicine, not to write notes optimized for DRG assignment — and she resents the queries from documentation specialists asking her to “clarify” the severity of a patient’s condition in language that happens to map to a higher-paying code.
The CFO sees it another way: coding is where revenue is captured or left on the table. A hospital on a 2-3% margin cannot afford to under-code. Every missed complication, every unqueried documentation gap, is money the hospital earned and never collected.
And the patient — the person whose suffering started this entire chain — carries whatever version of themselves the coder produced into every future encounter, every referral, every insurance decision. If the translation was accurate, the record reflects what happened. If it was distorted — by pressure, by haste, by an incentive pointing the wrong way — the patient carries that distortion forward, and may never know it.
The coder sits between all of them. If she codes conservatively, the CFO’s targets suffer. If she codes aggressively, the physician’s intent gets distorted and the patient’s record drifts from reality. If she crosses the line — and one in five has been pushed to — the False Claims Act exposes her to personal liability: treble damages, per-claim penalties, and the financial ruin that a $50K salary cannot absorb. The institution that applied the pressure negotiates a settlement. The coder does not have that option.
Ask anyone in healthcare operations what medical coding is for, and you’ll hear the same answer: it’s how we get paid. And that’s true. But it is also, if you step back far enough, a system whose incentives have learned to arbitrage revenue cycle games for profit — financial optimization layered on top of a clinical language that was meant to describe what happened to a person, not to maximize what a hospital collects for it.
R45.2 — Unhappiness
Every act of translation is a loss of fidelity. In 1956, Nikita Khrushchev’s “Мы вас похороним” was translated as “We will bury you” — a phrase that nearly defined the Cold War — when what he actually meant was closer to “We will outlast you.” One word shifted in register, and the gap between intent and interpretation widened into a geopolitical crisis.
Medical coders are translators — between what was meant and what gets recorded. They take the physician’s clinical language and render it in a language the payment system can process. The stakes are not geopolitical, but they are constant: thousands of dollars on each interpretation, hundreds of interpretations per week, tens of millions in revenue accumulating in the decisions of people making $24 an hour. A diplomatic mistranslation becomes a headline. A coder’s interpretation becomes the official record — the version of the patient that follows them through the system, that determines what they owe, what the hospital collects, and what shows up the next time a physician opens their chart.
Something is always lost in the crossing — a shade of meaning, a clinical nuance, the way a patient described what was wrong. When the translation is honest and the translator is protected, the loss is small. The system works well enough. When the translator is under pressure, the loss widens — and it widens in the direction of whoever is applying the pressure.
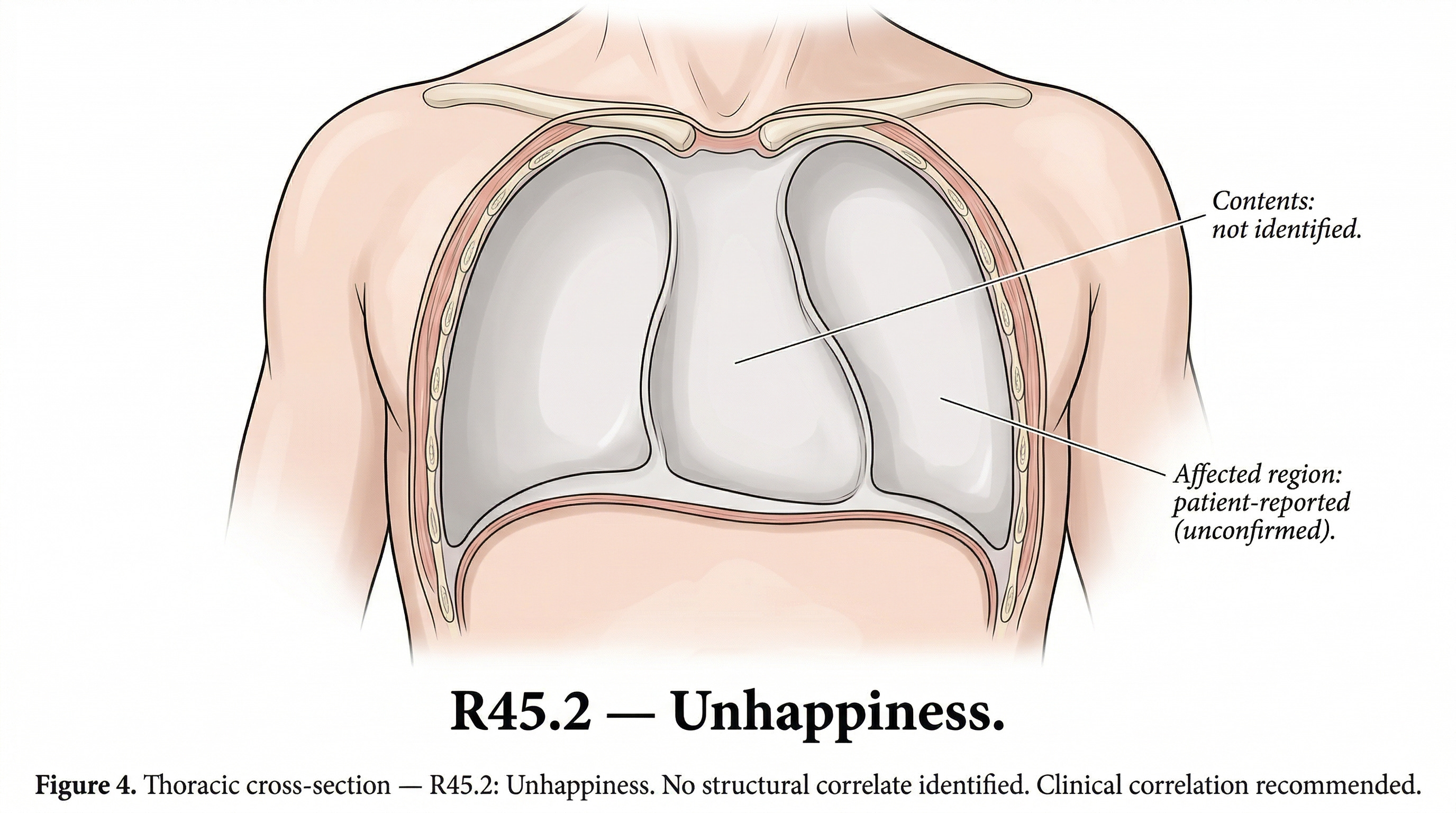
There is a code for “verbosity and circumstantial detail obscuring reason for contact“ (R46.7) — the patient who talks too much, who circles and digresses, who can’t quite say what hurts. The system noticed this and gave it a code. There is a code for “malingerer, conscious simulation” (Z76.5) — a billing category for faking it, which means the system that classifies disease also classifies the performance of disease. And ICD-10 code R45.2 is “Unhappiness”. Not major depressive disorder, not adjustment disorder — unhappiness, the feeling, given a billing code, placed between R45.1 (”Restlessness and agitation”) and R45.3 (”Demoralization and apathy”). Not every code moves money — R45.2 won’t swing a DRG. But a coder still has to assign it. The system still processes it. The feeling still has to pass through a clinical language and come out as data, whether or not anyone pays for it. The translation happens regardless.
A coder reads a physician’s note about a patient who is simply unhappy, translates that feeling into six characters, and sends it into the machinery. Whether the data that comes out still resembles the experience that went in depends on the state of mind of the person doing the translating, and the pressures she was under when she made the call.
We built an extraordinary machine of seventy-four thousand codes. A workforce of nearly 200,000. A woman on the aisle of Chris’s coding floor, who could read the clinical significance of a surgical complication and land on a ten-thousand-dollar outcome before the printer was fixed. The entire financial architecture of American hospital care rests on her judgment, and the entire pressure of that architecture pushes down on her desk. And every day she sits down, opens the next chart, and hopes the translation is close enough.
Everyone at the table benefits from more codes.
Specialty societies lobby for codes that distinguish their procedures — a distinct code means a distinct billing pathway.
Payers want granularity for fraud detection.
Researchers want it for outcomes tracking.
No one benefits from fewer codes.
James C Scott “Seeing Like a State” but for healthcare.
This is so well done! So true: Every act of translation is a loss of fidelity.