

3.3k words, 13 min read
Editor's note: This is the 2nd of 5 essays in The Cycle, my series on healthcare's revenue cycle. Ongoing writing to continue here.
I couldn’t seem to attribute the source, but auto repair shops have had this joke since the 70s:
Fast, Cheap, Good: Pick two.
With five simple words, the punchline illustrates the idea of real-life constraints. Yet I’ve always wondered: who wouldn’t pick Good?
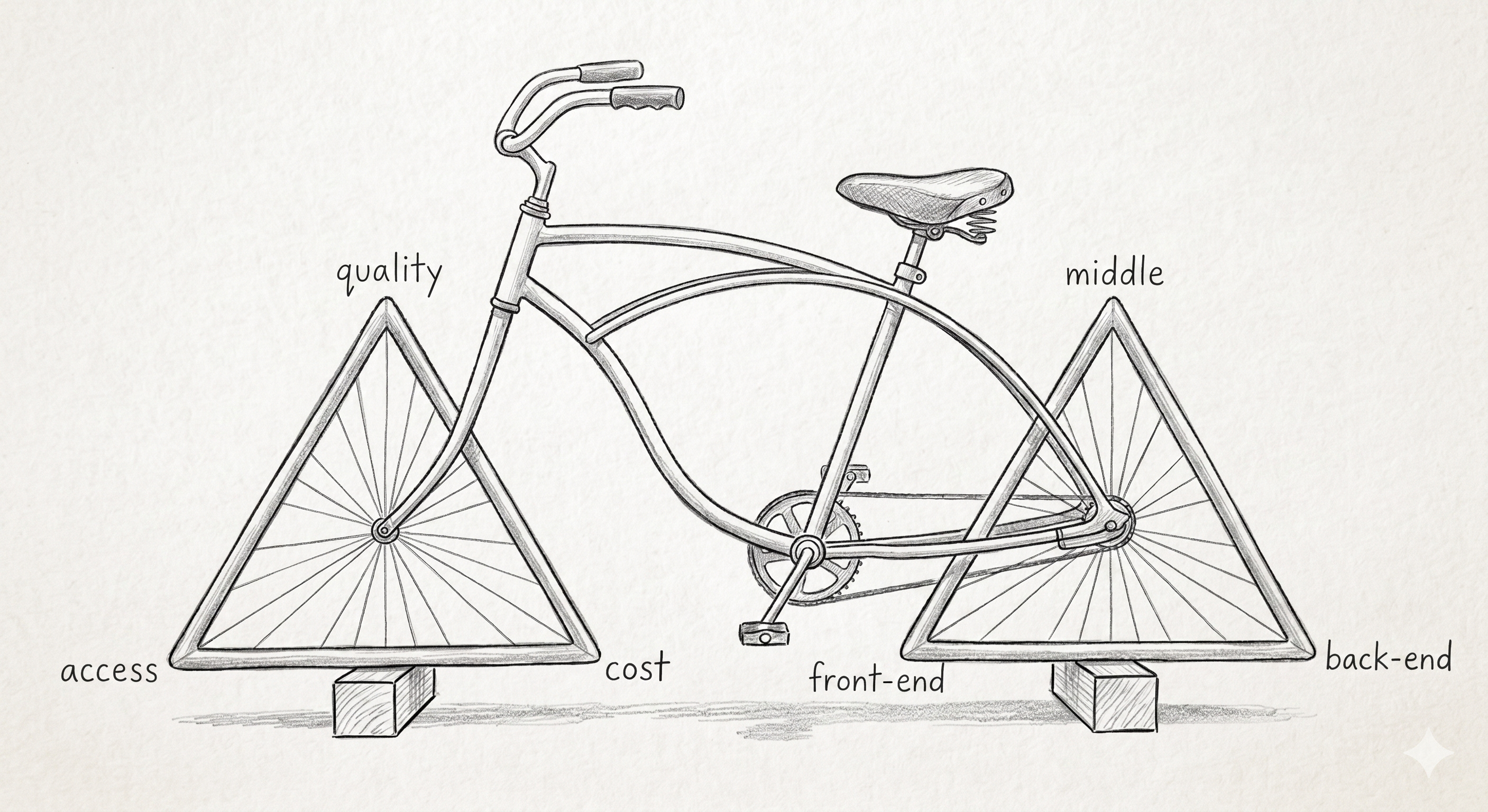
It’s a popular idea that spans trades and industries. Engineers built a discipline around this concept and called it the project management triangle, showing the same trade-offs. And in the 1994 book Medicine’s Dilemmas, Dr. William Kissick — a drafter of the original Medicare legislation — named the healthcare version of this: the Iron Triangle, a trilemma of Access, Quality, and Cost. You can have a system that does well at two of them, not all three.
The cruelty of the choice is that Quality is the corner you can’t really trade off. A lower-quality replacement part for my car wears down a few years sooner - which is annoying, but acceptable. A lower-quality stent in a heart valve is not a trade I’d take. Settling for lower-quality healthcare feels foolish, which means the triangle has to bend on the other two - access and cost. Someone gives up the appointment, or someone eats the bill. The triangle isn’t really about three properties; it’s about which trade-off is most acceptable.
Revenue Cycle as a Triangle
The triangle reads as a policy abstraction. But it gets decided every day, in millions of small decisions, by people who do not think of themselves as policymakers - registration clerks, eligibility specialists, coders, claim scrubbers, denial managers, billers, collectors. The apparatus they work inside is the Revenue Cycle - the financial process in which a patient’s encounter is scheduled, documented, and finally paid. There are three distinct phases: front-end before the encounter, middle during it, back-end in the months after.1
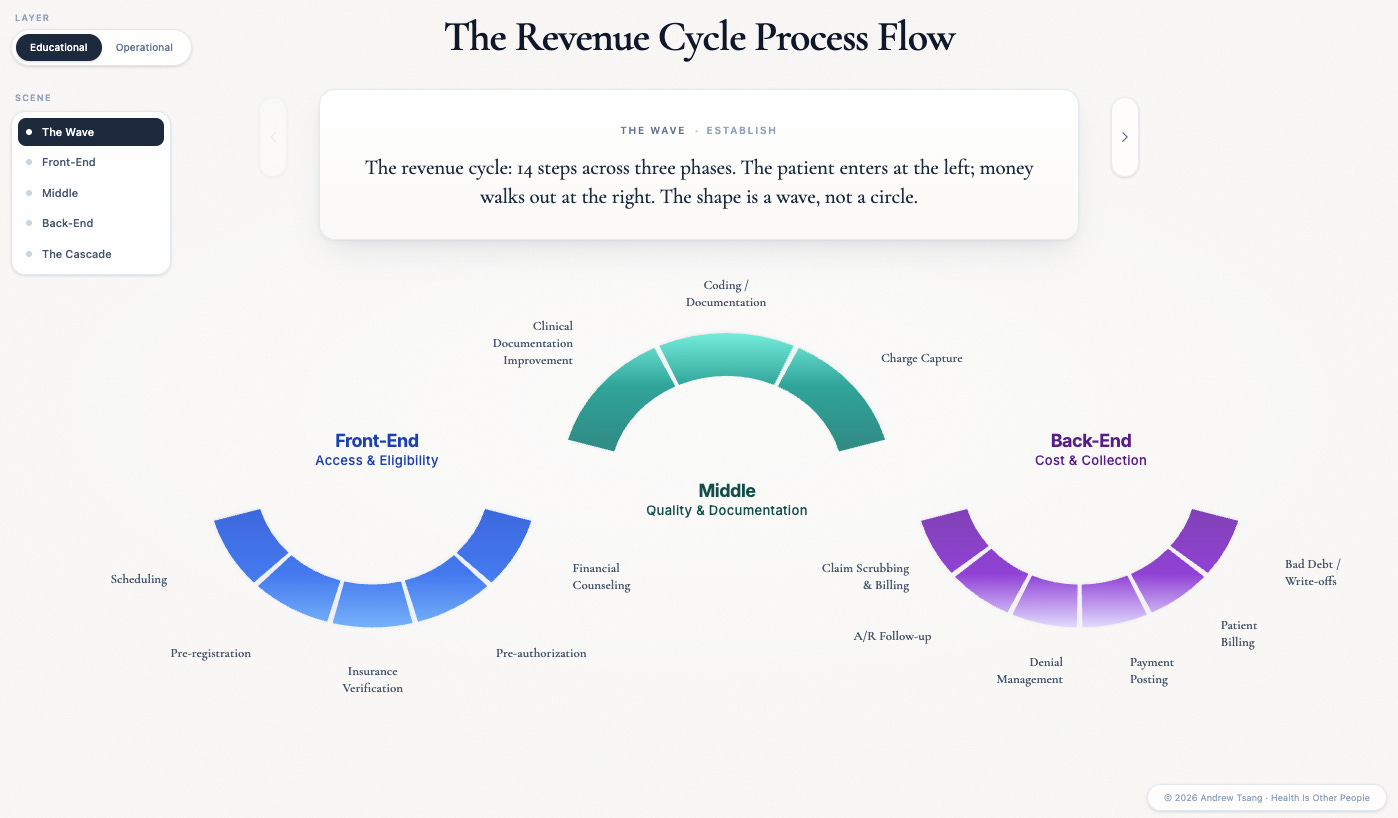
Hover over one of the steps and watch the ripple. The shape isn’t a circle, despite the name - a patient enters from the left, but money walks out on the right. Each phase in the revenue cycle directly affects access, quality, and cost - the central trade-offs in American healthcare.
I’ve seen a lot of healthcare claims, and every claim is a small case study in this trilemma. Most people see boring forms and numbers; I see a story. With nothing but a stack of claims and remittances, I can trace the ups and downs of a patient’s life — what they tried to do, what got in the way, who paid, who didn’t, and who got hurt by the gap in between.
Let me walk you through one. A 52-year-old finally scheduled the colonoscopy her PCP had been nagging her about. Under the Affordable Care Act, screening colonoscopies are preventative care - the patient pays nothing if everything goes according to plan. She thought hers would be free, and on paper she was right. As we trace the case forward, you’ll see how she ended up wrong.
Front-End = Access
From the first step of booking her appointment, our patient begins her journey on the Front-End of the revenue cycle - sometimes called “patient access”. On paper, she does everything right: appointment booked, eligibility checked, no prior auth required at this age, appointment confirmation call, prep packet, clear-liquids sheet, all green lights. But the front-end exists because almost nothing in healthcare goes according to plan.
Two things have already gone wrong that will cascade into months of headaches. Registration entered her insurance information from a photographed card and got one field wrong - a subscriber number off by a digit, enough to break eligibility downstream. And the procedure was booked under the assumption that nothing about the encounter would change during the procedure. Mistakes like these are how routine front-end work becomes the back-end’s problem six weeks later.
This is the Access phase, and its decisions echo through the entire cycle. The wrong field in registration becomes the denial in week six. A prior auth obtained for the wrong code becomes the appeal that ties up two FTEs for a quarter. Front-end work decides who gets care - and decides, in advance, most of what happens to the claim downstream, which has real patient consequences. According to an AMA survey, 34% of physicians watch patients abandon treatment after a prior-auth fight. Each step in the onerous process deters patients from accessing care.
Every step before the procedure is a small bet against something going wrong later - and when those bets lose, the cost doesn’t disappear. It moves to whoever is standing closest to the problem.
Middle = Quality
The procedure goes as scheduled. Under twilight sedation, the gastroenterologist finds two polyps - snares them, drops them in a specimen jar, and sends them to pathology. To the patient on the table, the procedure still feels like the screening she came in for. But on the operative note the doctor writes up afterward — the clinical record of what actually happened in the room — the encounter has already changed. From the dashboard view at the end of the week, this case will look identical to the forty other colonoscopies that ran the same day, until a coder opens that note three days later.
The instant those polyps are biopsied, the encounter changes from screening to diagnostic - different CPT code, different billing rule, different patient liability. Three days later, a coder sitting at a screen forty miles from the procedure room opens the operative note. She has to decide whether to append modifier -332 — a two-character tag added to the billing code, marking the procedure as preventative so the payer keeps treating it as a screening for cost-sharing purposes. A month’s rent is sitting on the knife’s edge of that two-character decision. If the coder appends the modifier, the patient still owes nothing. If she misses it, the patient owes $1,840 — a bill set in motion by someone she will never meet, based on a billing rule she has no idea exists.
This is the Quality phase, and the word is doing strange work. Quality in revenue cycle is not the same thing as clinical quality, but they’re directly related: it’s not whether the patient got better, it’s how accurately the encounter is rendered on paper. The middle is where the clinical reality the doctor experienced gets translated into the billable artifact the payer will see. What was this encounter? The coder’s answer flows downstream into the payer’s records, the appeal queue, and the patient’s bill — and you only get to answer it once.
What the middle decides is what the back-end inherits. The coder’s modifier choice will determine whether the appeal three months from now is a fight or a formality. The coders, the documentation specialists, the charge auditors — they’re not setting healthcare policy. They are deciding patient experience, one encounter at a time.
The claim goes out. A clean claim, in revenue-cycle speak, is one the payer accepts on first read — no missing fields, no codes in conflict, no eligibility mismatches — and about 84% of claims at a typical hospital clear that bar. This one will not. Two assumptions from week one are about to come due in week six, and the burden of resolving them is about to land on someone else’s desk.
Back-End = Cost
The Denial
Two weeks later, the denial comes back. The patient will not hear about it for another six weeks - she will be eating Thanksgiving dinner with the bill she does not know about sitting in a folder on her counter. The hospital hears it immediately. In the 835 file — the clunky, electronic remittance file, which uses the EDI (Electronic Data Interchange) format designed in an era optimized for kilobytes3 — the denial is a single row of text:
CARC 31. Patient cannot be identified as our insured.
CARC stands for Claim Adjustment Reason Code - there are over 200 of them in active use. Code 31 is the insurance company’s reading that they have no record of this person under this plan, and that single row is the entire communication: no human voice, no explanation, no record of why. Behind it is the subscriber number off by a digit from registration day — the insurer can’t find her — so the claim is rejected before the modifier-33 question even matters. One row of data, a month of human labor to reverse it, and $1,840 the patient owes until that work is done.
The denial management team picks up the case on the other end. Tier 1 work — the templated denials with known patterns and known fixes — is handled by a vendor in Manila, twelve time zones from the hospital’s billing office, working through queues that already have a few thousand items in them when the shift starts.
Outsourced revenue cycle is mostly arbitrage: cheaper labor doing predictable rework, which works well for templated denials and breaks at the edges where context matters — the unusual modifier, the half-documented op note, the eligibility detail that doesn’t match anything in the playbook. The mismatch from registration day, fortunately for everyone, is exactly the kind of thing they look for. They request medical records to support the modifier-33 documentation, attach them to the case, and file an appeal. The appeal cycle is slow: twenty to forty days, depending on the payer. The cost to file — staff time, documentation pulls, follow-up calls — runs $45 per claim. Across the industry, roughly half of appealed denials get overturned on the first try; with persistence, around two-thirds eventually get paid.
Meanwhile, the patient is about to find out about the bill. The cost of resolving it is already mounting - just on someone else’s ledger.
Job to be Done
A letter arrives in the mail.
Your insurance has determined that this service is not covered under your preventative benefit and you are responsible for $1,840.
It’s wrong (not just morally), but she doesn’t know it’s wrong. She doesn’t know what an EOB is — that it’s a notification, not a bill — and the document was not designed to clarify the difference. So she calls the insurance company. They tell her to call the hospital. She calls the hospital. Patient billing tells her the claim is in appeal and please don’t pay anything yet. Then patient billing, running on its own schedule, mails her a statement because the system flagged a balance. Three departments at two organizations are now arguing on her behalf about $1,840 — hours of paid labor at the hospital, hours of unpaid labor by her, all of it set in motion by a mis-typed subscriber number from week one.
Unfortunately, neither the insurer nor the hospital will be able to help her through this easily. The work of navigating this system is a job-to-be-done, but nobody is incentivized to pay for this to happen.
The Cost of the Cost
The industry has a name for what hospitals spend just to get paid: cost to collect. In 2024, US hospitals spent roughly $43 billion on it, per the American Hospital Association — money for staff, software, vendors, and appeals that never touches a patient.
For a mid-sized academic medical center, that’s hundreds of FTEs, tens of millions of dollars a year, and a building full of people whose entire job is chasing claims that should not have been denied in the first place. Every quarter, the hospital submits tens of thousands of claims, watches an industry-average 11% bounce back as denials, and runs a back office sized to fight the rest back into payment. None of those numbers describe a hospital in distress. They describe an average hospital, on a Tuesday, handling its share of the roughly 500 million claim denials American insurers issue annually. The cycle does not look like a crisis from the inside. It looks like a job.
This is the Cost corner of the triangle, and it isn’t the cost of the procedure — it’s the cost of deciding who pays for it. Almost all of it is invisible to the patient who started the cascade by mis-typing a subscriber number. The rest gets folded back into premiums and bills, paid in small increments by everyone else who carries the system’s costs.
Resolved
As we reach the resolution of this claim, nearly twelve weeks after the procedure, the appeal lands. The hospital eats most of the difference; she owes the coinsurance her plan attaches to a diagnostic procedure. She pays $200 — less than the $1,840 the letter threatened, more than the $0 the ACA promised. The final statement reads balance: $200. And while she doesn’t know what changed or why, she is not scheduling another preventative appointment any time soon. Something about the word free in the preventative care that she has sworn off.
Front-end, middle, back-end. Access, Quality, Cost. And our patient got access and quality, but has paid the cost: first in dollars, then in trust.
Another Iron Triangle
Now turn the triangle.
The corners we put on the slide — Access, Quality, Cost — describe what’s getting traded off. They don’t describe who’s doing the trading. Behind each one is a person who absorbed a share of the $1,840 colonoscopy we’ve just traced.
The patient wanted fast access to preventative care that was supposed to be free, and walked away owing money she hadn’t budgeted for - because a subscriber number was off by a digit on day one.
The provider delivered good quality care, and had to trust that a coder forty miles from the procedure room would translate two polyps into a billing code that survived a payer’s review.
The payer wanted cheap cost for the care, and answered the claim with a single line of CAR code - then spent a month watching a denial team drag it back into payment anyway.
Patient, provider, payer — three parties, each capable of bearing some share of the load, with a constraint that the load has to fall on at least one of them. The cycle is the apparatus that moves it between them.
Every fix-the-revenue-cycle initiative I’ve worked on hits the same ceiling. You can scrub claims cleaner, deny less aggressively, schedule more efficiently, code more accurately. You can deploy AI on either side of the payer/provider line and shave a few days off A/R. What you cannot do is make all three parties’ lives easier at the same time. Burden of work is conserved.
Exceptions that Prove the Rule
To steelman my metaphors, there are two objections worth addressing.
The first: there are really more than three parties. Behind every payer stands an employer (commercial coverage) or a taxpayer (Medicare and Medicaid), and the load the payer absorbs eventually flows back to them as premiums or taxes. Factually correct, and it strengthens the metaphor instead of weakening it. The employer paying premiums doesn’t see the denied claim. The taxpayer funding Medicaid doesn’t see the appeal (neither do I). The patient sees the EOB but can’t read it. Meanwhile, the hospital’s denial team and a payer’s medical director negotiate a roughly $1,800 line-item on a first-name basis. The system keeps the people most exposed to the load farthest from the work that decides who eats it.
The second: the trilemma is an artifact of US payment fragmentation. Single-payer countries don’t have it. Kaiser doesn’t have it. Eliminate the cycle and the constraint disappears.
The cycle disappears, but the constraint doesn’t. Integrated and single-payer systems internalize the load instead of litigating it, constrained by the same triangle but at a different angle:
Access — NHS England. NHS England doesn’t run prior-auth fights, but it does ration access - through wait times. The elective list peaked past 7.5 million patients in 2024. The access constraint exists in single-payer just as it does in fee-for-service; it just looks like a queue instead of a denial.
Quality — Kaiser Permanente. Kaiser is integrated payer-provider, so the medical-necessity decision happens inside one wall instead of across two. The trade-off about which procedures get approved still gets made - by Kaiser’s physicians, using Kaiser’s protocols. Integration doesn’t eliminate the gatekeeping, it merely relocates it.
Cost — Canada. Canada’s provinces don’t run claim denials, but they do ration cost - but it’s upstream, through formularies, wait times, and provincial capital budgets that decide which hospitals get which scanners. The cost trade-off happens at budget time, not at billing time.
Integrated and single-payer systems do shrink one part of the load — the deadweight of two organizations litigating the same claim goes away when there’s only one organization. The underlying constraint doesn’t. The iron triangle isn’t an artifact of US payment fragmentation; it’s the geometry of finite-resource healthcare itself. Pick a system and you can see which corner it bends. You won’t find one that bends none of them.
Try Angles
Back to the United States, where the cycle is the apparatus. There are three configurations, and all three are hard:
Easier for the patient. The load moves to the payer-provider fight. The fight gets longer, more expensive, more byzantine. The patient gets a smoother experience and a more opaque one - no real idea what just happened, who paid, or what she would have owed.
Easier for the provider. The load moves to the payer (who tightens the screws) and to the patient (who absorbs more of the friction by filling out more forms or confirming more appointment reminders). This is what happens when a hospital outsources its revenue cycle to a third party with aggressive collections.
Easier for the payer. The load moves to the provider (more documentation, more denials to appeal) and to the patient (more coinsurance, narrower networks, more prior-auth steps).
You’ll notice I haven’t written a fourth option: there isn’t one. You can grow the pile, which is roughly where the country has been heading for thirty years, or shrink one party’s load by moving it to another desk (basically what I do at work to improve my productivity).
This is why “automation will fix the revenue cycle” doesn’t quite work. Some specific frictions do shrink. Real-time eligibility checks prevent denials from getting written. Electronic remittance advice eliminated a category of paper that used to consume FTEs.
But the last decade of automation has mostly moved the pile, not shrunk it. Payers automate denials; providers automate appeals; the work goes faster, the work is still there. HFMA calls the pattern the battle of the bots. Whoever automates faster sends more load to the slower party’s desk. Total cost — in dollars, hours, patient anxiety, and clinician moral injury — has not fallen.
There is an unstated problem here: if you want it easier for the patient, the payer and the provider have to absorb more of the load - and neither has any structural reason to. The American revenue cycle is what you get when no one with the power to shrink the pile is paid to shrink it. Payers are public companies with margin targets. Providers are squeezed between rising labor costs and flat Medicare rates. Patients have no leverage individually, no lobby collectively, and no clear path to push back. The people who could change the cycle are the same people who would lose if it changed.
So the next time you read about a fix — a new AI tool, a payer initiative, an interoperability mandate, an EHR upgrade promising to “transform” the revenue cycle — don’t ask whether it works. Ask which party absorbs the new load, and whether that party has any reason to.
This oversimplifies the complexity of the Revenue Cycle, which is often misunderstood as just a back-office admin function. When I worked in healthcare consulting at Deloitte, we ran a four-day bootcamp with 200+ slides just to onboard new analysts to it. Fourteen steps, give or take depending on the system, all interdependent — the front-end is everything before the encounter (scheduling, eligibility, prior auth, financial counseling), the middle is the brief window where the encounter gets documented and translated into a billable claim (coding, charge capture, clinical documentation improvement), and the back-end is the uphill slog of resolving that claim through scrubbing, A/R follow-up, denials, appeals, payment posting, patient billing, and write-offs.
Modifier -33 was added to CPT in response to the ACA’s preventative-services-cost-sharing requirement. The ACA created a rule — preventative services must be free to the patient — that the existing billing system was not built to enforce. Modifier -33 is the system’s way of marking this counts as preventative even when it does not look that way on paper. Every time a coder appends it, she is resolving a regulation in real time.
You can’t imagine how many of these files I’ve squinted over in my early days doing RevCycle consulting. The file format is an affront to God.
{kind=link}
I love how this reads almost like a horror film… reminds me of the movie Brazil where the main character’s whole life spins into disaster because of a typo!
The mention of "Colonoscopy" and "Denial" is bringing me back to my last colonoscopy, which was a few years ago, back when I had an ACA plan (before aging into my Medicare-for-Me plus Medigap).
So, the anesthesiologist's office apparently put in the wrong code, and the claim was denied. A call to the insurance company did not resolve this, despite me pointing out that the anesthesiologist's service was dated the exact same data as the colonoscopy by the gastroenterologist, which gastroenterologist bill was approved.
So, I had to do a formal appeal to the insurer, and write lots of details down on a form.
(Which did get the anesthesiologist contacted, the bill altered to the correct code, and the claim approved.)
--
I note that both the insurer and the hospital where the procedure was performed are non-profits. It makes little difference--the problems for patients are still there.
It is a fallacy commonly observed in Substack comments that the problem is the for-profit stuff. (Fortunately, I have a video by former ER doc and current health care journalist Elizabeth Rosenthal making the point that not-for-profit does not solve our problems:
https://www.youtube.com/watch?v=7mdIwgwBBgY&t=680s
Her focus is the problem of people waiting for hours or days in, or in the halls just outside of, ERs, waiting for a bed to be admitted, but I have the video pointed to where she makes that point about not-for-profit not saving us.)