
The Other People on the Seesaw
Trade-offs between stakeholders on our healthcare seesaw


There was this cynical joke when I started in healthcare finance consulting: from the moment you're born, you're a patient - and you get a hospital bill to prove it.
That dark humor captures something real about how we think about healthcare reform. Everyone starts as a patient, which is why most proposed solutions are “patient-centered”. But after fifteen years bouncing between hospitals, insurance companies, pharma, tech, and a little policy - I've learned that other stakeholders in the American healthcare system have their own challenges and incentives.
So I modeled this serious, complex system of imbalanced power dynamics into an advanced framework: the Healthcare Five-way Seesaw (a serious name, I know).
The Seats on the Seesaw
Every complex system serves multiple constituents. In a system of law, stakeholders include citizens, police, courts, and lawmakers. In an economic system: businesses, workers, consumers, and regulators have differing incentives that serve to push the goals of the overall system forward.
Healthcare has five main constituencies: Patients, Providers, Payers, Government, and Suppliers.1
To see how this plays out, let's look at where each group sits on the seesaw right now:
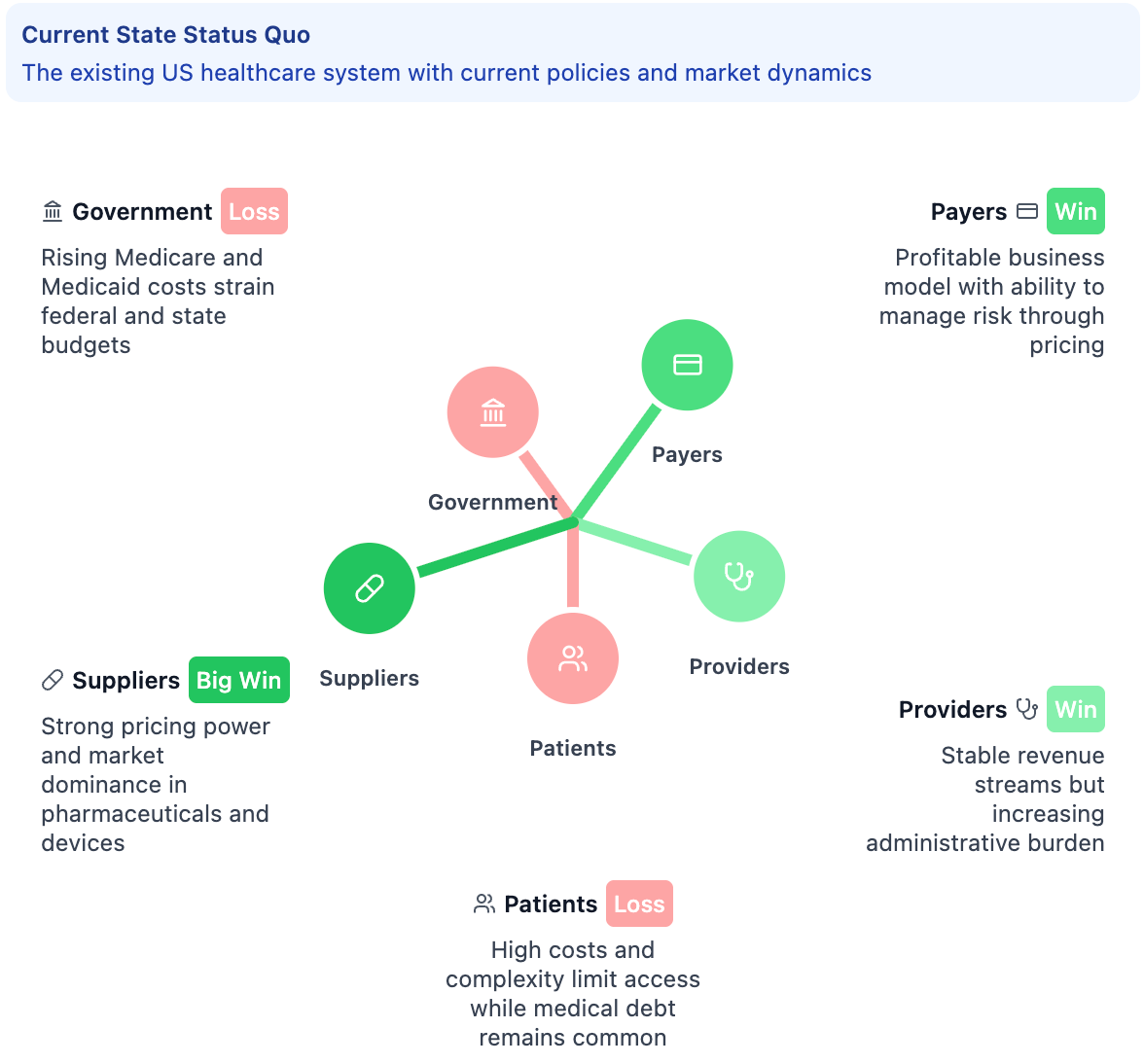
These stakeholder groupings each react differently to the same health policy, the same innovation, the same market dynamics. Some will win, some will lose, some are born to sing the blues. But the second- and third-order ripple effects will go on and on...
Let’s explore each stakeholder to learn more about incentives and challenges:
Patients: The People Healthcare is Supposed to Serve
We the Patients are the center of healthcare, but we have the least control over what happens to us. Patients are the only “customers” who regularly get services they didn't ask for, can't refuse, and don't directly pay for. If your appendix bursts, you’re not comparison-shopping emergency rooms. You go where the ambulance takes you, get whatever treatment the doctor orders, and hope your insurance covers it.
Let’s see how this plays out when the balance shifts - say, through hospital price transparency where patients can finally comparison-shop for procedures.
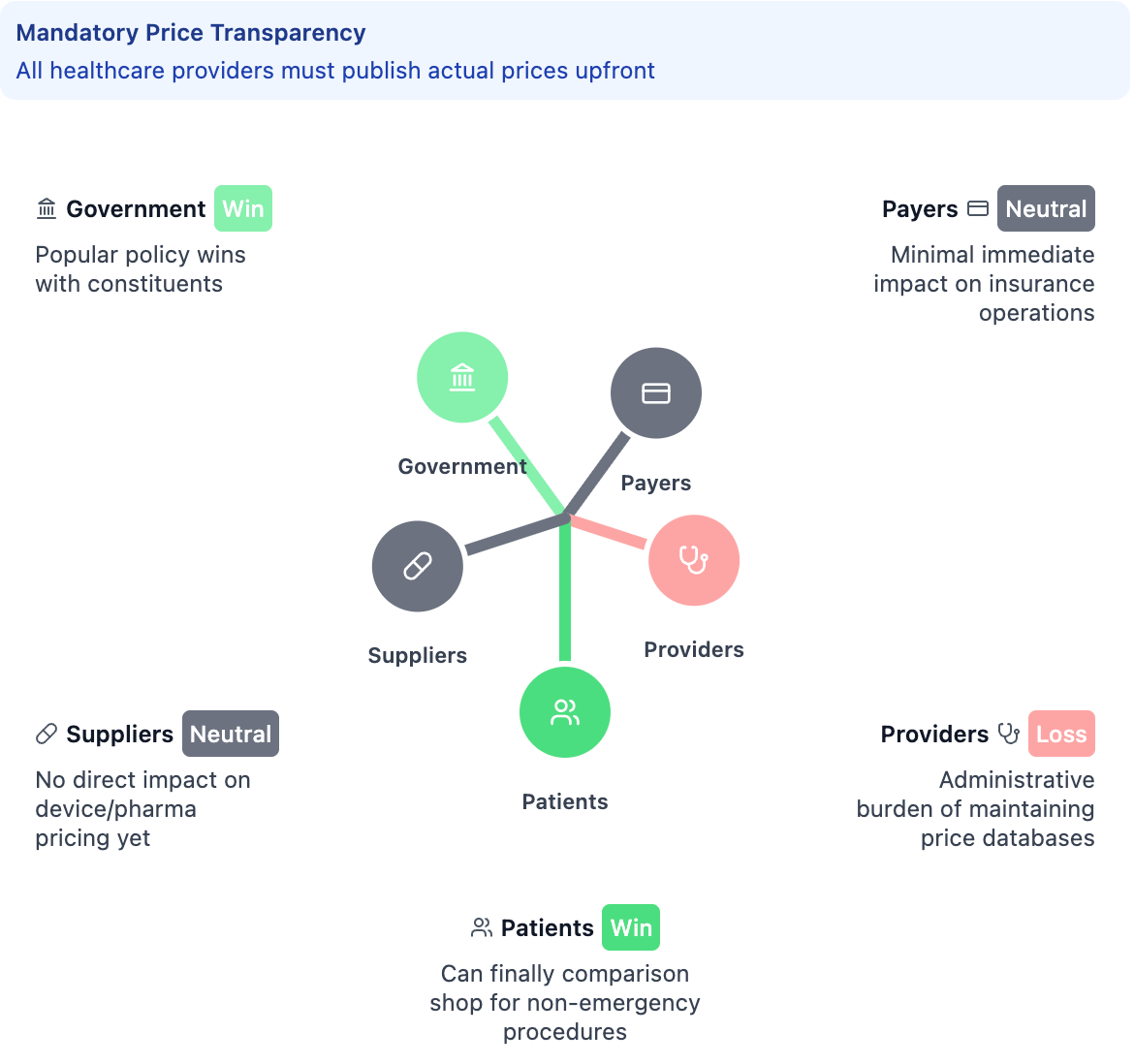
In the immediate term, you can see how patients move up while providers get pushed down - but notice how Payers and Suppliers stay relatively neutral. But providers worry about price wars cutting their already-thin margins, which puts hospitals at risk and could harm patient access. Payers and Pharma may even out in the near-term, since operations are largely unimpacted…
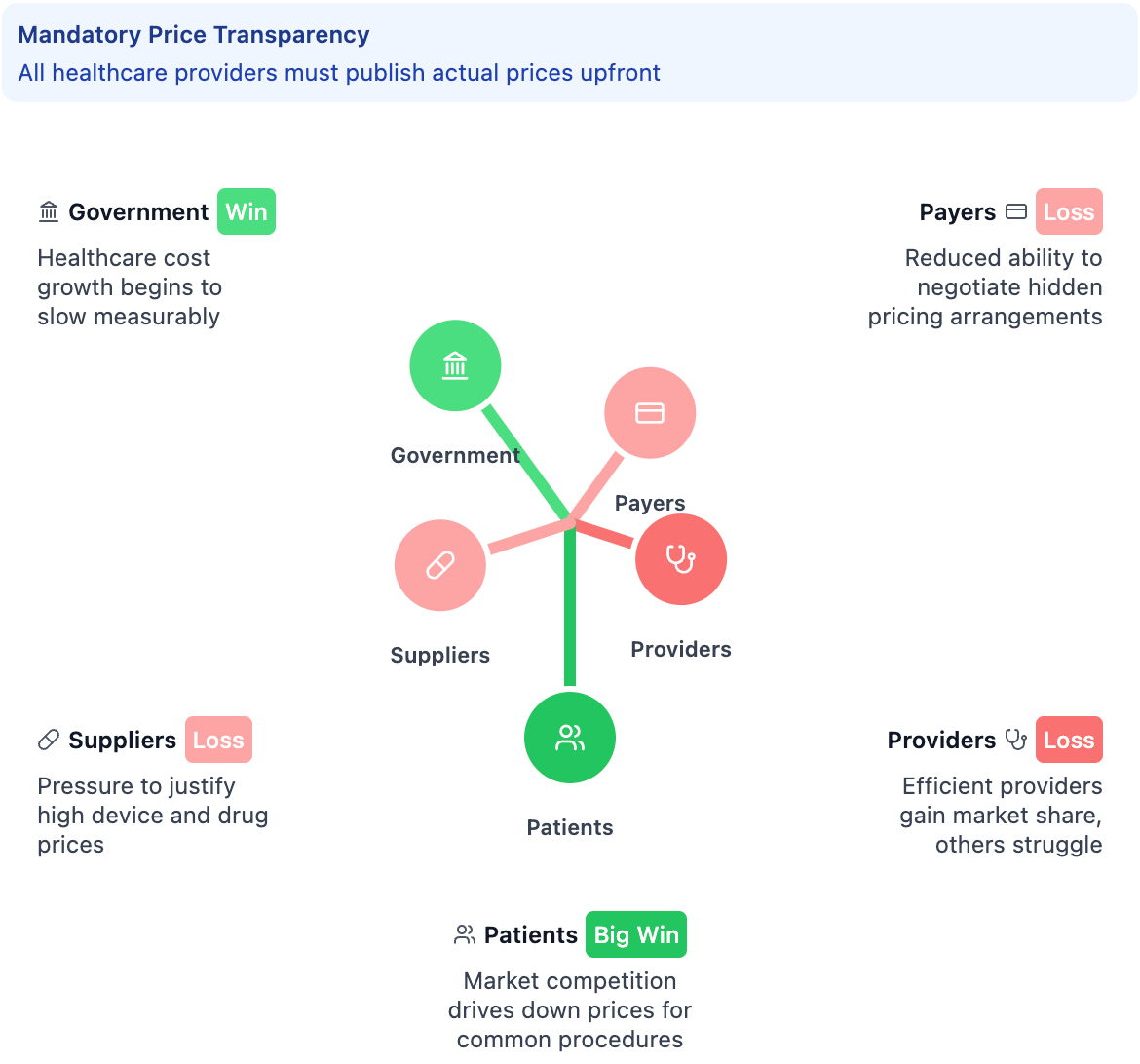
…but Payers and Pharma may lose negotiating leverage since everyone can see the real rates in a longer-term horizon. Suppliers face pressure to justify their pricing. The five-year view shows how the secondary effects kick in - now payers and suppliers are getting squeezed as the transparency creates new market pressures they didn't anticipate.
It’s arguable that in the current U.S. healthcare system, the seesaw is most imbalanced away from the patient. However, that’s not always the case: patients are becoming increasingly savvy consumers - doing their own research, demanding better experiences, and taking more control of their health. Big wins are sorely overdue for the patient, there are trade-offs to other stakeholders to consider.
Providers: The People Who Actually Deliver Care
Every medical director I’ve come across has run into same problem: “They want my staff to have higher quality scores AND higher patient volume with the same resources.”
That's healthcare Providers in a nutshell - caught between wanting to help people and needing to make the numbers work, with everyone assuming they can somehow do both perfectly.
This group includes everyone from neurosurgeons pulling down $2,000 an hour to nursing assistants making $20/hour in a retirement home. They all technically “provide care”, but face completely different pressures. Even where they are employed changes their incentives: the doctor at a hospital balances productivity against patient satisfaction (volume vs quality), while the independent doctor worries about keeping the lights on while insurance pays them less each year.
This seat on the seesaw can get out of balance quickly with the wrong policy: Government quality metrics might improve care standards, but require providers to hire data analysts instead of nurses. Patient demand for convenience might drive telemedicine adoption, but reduce the personal connection that makes providers most effective.
Providers are also the best positioned to fix healthcare's problems because they see where the waste and inefficiency actually occur. Generally the best healthcare is where providers have the most input in the system - that is, when they are aware of the other parts of the system.
Payers: The People Who Pay the Bills
This is where healthcare gets confusing, even for insiders. The term Payers - in layman’s terms - usually refer to health insurance. But that's oversimplifying it. Your “payer” might be a massive insurance company, your employer who pools funds to provide employee benefits, or government programs like Medicare and Medicaid - each operating under completely different rules and pressures.
Think of payers as risk managers, which is essentially just a bet. They collect money today (premiums) and bet that it will be enough to pay for expenses later (medical claims). They make money when people don't use healthcare, which puts them at odds with literally everyone else in the system.
The seesaw dynamics are most prominent here: When payers move up - say, through higher deductibles or prior authorization requirements - healthcare costs might stabilize and risk is better managed… but patients face more financial barriers and out-of-pocket costs, providers deal with administrative overhead and delayed payments, suppliers face coverage restrictions that limit market access, and government officials field complaints about access problems.
When other stakeholders push back against payers, the math gets messy fast. Patient advocacy for coverage mandates - say, covering pre-existing conditions - means higher medical costs that eventually flow through to premiums. Government regulations like essential health benefits expand coverage, but increase baseline costs. Supplier innovation creates new treatment options that patients want covered, putting payers in the position of either saying no to medical progress or raising everyone's costs.
The real problem isn't that payers exist (or that we have a multi-payer vs single-payer system). They get a bad rap because they have to say no when it comes to healthcare spending. Resources are finite, yet healthcare demand is essentially infinite. The payers are put in the position of saying “no” because no one else can.
Government: The People Who Make the Rules

The next constituent is the Government, or in this case, policymakers and regulators. The government sets the rules for how healthcare works, but those rules often have unintended consequences that ripple through the entire system.
Government also wears multiple hats in healthcare. Sometimes it's the regulator (FDA), sometimes it's the payer (Medicare and Medicaid), sometimes it's the provider (VA hospitals), and sometimes it's all three at once.
This creates hilarious contradictions: The FDA wants drugs to be safe and effective, which takes time and money. CMS wants healthcare to be affordable, which means paying less. The CDC wants to prevent disease outbreaks and improve population health, which requires more reporting and surveillance. These are all reasonable goals that work against each other.
When the government decided that hospitals should be penalized for patient readmissions, suddenly every hospital in America started calling patients at home to make sure they were taking their medications. Good for patients (better follow-up care), challenging for providers (new administrative burden), neutral to positive for payers (fewer expensive readmissions), but it created a whole new market for suppliers building patient engagement technology.
Government also moves like a glacier in a world that needs quick fixes. When Medicare decided to cover annual wellness visits, millions of seniors got preventive care. A noble aim, but it took years to implement and created new administrative overhead that providers are still complaining about.
The thing is, Government is also healthcare's most powerful force for positive change to realign incentives across the whole system - which makes every regulatory change a potential earthquake for the other four corners.
Suppliers and Innovators: The People Who Build Healthcare's Tools

One of the most obvious, but also overlooked, parts of the healthcare system are the Suppliers and the innovators. For this framework, I lumped everything into a pretty big category, but basically it's the stakeholders creating the tools or the medicines or the technologies that help providers give care. So this can be pharma, biotech, health IT, medical devices - anything that kind of feeds into the supply chain of healthcare.
My experience in pharma and health IT have shown a similar pattern: the aim is to speed up innovation with expensive bets - but the payoff of that bet depends on your perspective. A pharmaceutical company might spend $2.6 billion developing a new cancer drug that extends life by six months. Is that worth it? The patient facing cancer says absolutely. The insurance company looking at costs says maybe not. The doctor says it depends on the patient. The pharmaceutical company says they need to recoup their investment or they can't afford to develop the next drug.
But when other stakeholders push back against suppliers, the innovation equation gets complicated. Payer formulary restrictions might control costs, but limit patient access to newer treatments. Government price controls might make drugs more affordable, but reduce R&D investment for future innovations. Provider consolidation creates fewer, but more powerful buyers who can negotiate volume discounts - great for Epic selling to major health systems, brutal for smaller health IT companies trying to get innovative pilot programs off the ground. Patient advocacy for faster approvals might speed access, but potentially compromise safety testing that took years to design.
Therefore, suppliers and innovators are constantly balancing three competing pressures: clinical effectiveness (does it work?), economic viability (can we afford to make it?), and market acceptance (will providers use it and payers cover it?). But when this balance works well, you get genuine breakthroughs - like insulin pumps that automatically adjust dosing, or AI systems that can spot cancer earlier than human radiologists.
It’s easy to complain that healthcare innovation happens slowly - but having been inside pharma and health IT, it’s slow because the stakes are so high. You can't beta test a pacemaker the way you beta test a social media app. People's lives depend on this stuff working perfectly the first time.
Disclaimer
Obviously each of these groups contains multitudes - this is not meant to be a mutually-exclusive grouping - but this best shot at a comprehensive framework illustrates the major fault lines.
When the Seesaw Tips
The thing about complex systems is that there are second- and third-order effects you can't see coming. With a regular seesaw, you might eventually find balance. With a five-way seesaw, every movement creates reactions across all corners that nobody predicted.
To make this more than just theory, I built an interactive simulator that lets you test healthcare scenarios before they become trillion-dollar policy experiments. You can input any scenario - Medicare for All, telehealth expansion, drug pricing reforms - and explore how each stakeholder group might respond over different time horizons.

Watch how it affects all five stakeholder groups simultaneously - immediate effects, five-year impacts, ten-year consequences. Play with the prototype here.
Look, I'm not claiming this thing predicts the future - healthcare is way too messy for that (and honestly we might as well be trying to forecast the stock market). But what it does is make you consider stakeholder perspectives you probably weren't thinking about - the ethos here at Health is Other People.
When you input “Medicare for All”, it doesn't just show you the obvious effects on patients and government. It makes you think about how providers would handle new payment structures, how insurers would reshape their business models, and how pharma companies would deal with negotiating against a single massive customer.
Finding Balance
Most “fixes” in healthcare just move problems around - shifting costs from patients to providers, from payers to the government, from this year’s budget to next year’s health crisis. But every major change in healthcare raises the same questions: Who wins? Who loses? What are the unintended consequences? And when the stakes are life-or-death, how do you actually implement changes without breaking something else?
The rare wins create positive outcomes for multiple stakeholder groups both immediately and long-term, but those are hard to find and harder to implement.
This Five-way Seesaw framework helps explain why healthcare reform is uniquely difficult. Policy proposals aren't just about helping patients or controlling costs - they’re about managing competing pressures across five different groups with fundamentally different incentives.
The most important industry in America runs on stakeholder dynamics that shape everything from the health economy to your doctor's appointment availability. Understanding those dynamics doesn't solve healthcare's problems, but it might help explain why solving them is so damn hard.
Two things:
a.) This isn’t a novel idea - others have done primers on US Healthcare in different ways. I also recommend the great Halle Tecco’s Pepe Sylvia breakdown.
b.) I really wanted to call it Policy (instead of Government) and Pharma (instead of Suppliers) to get the 5 P’s. For Suppliers, the focus is innovators, so I’ve lumped pharma, med devices, and health tech together in this category.
Love the idea, this could probably be improved through trying to cite real evidence and not just ~vibes~.
E.g. for "Medicaid Work Requirements", the 'Patients' section said "Some patients find employment and coverage stability, but many remain uninsured with delayed care needs."
This just ignores the evidence from states like Arkansas that implemented Medicaid work requirements that 90%+ of people who lost coverage actually qualified, but were overburdened by the paperwork or didn't realize they needed needed attestations. Unemployment in Arkansas actually went up in the population, as some people with jobs got cut from Medicaid, couldn't get medical care, and then because of illness lost their jobs.
This is a fantastic post!