
I Believe The Children’s Hospitals Are Our Future
The Medicaid cuts are designed to shrink government’s role. Children’s hospitals show why they’ll do the opposite.

3.7k words, 15 min read

In March 2025, politicians and hospital leaders held a press conference at the Enders Research Lab where they helped cure polio - not to announce a breakthrough, but to push back against the 24-hour news cycle coming out of Washington. Standing at the podium next to the governor was Dr. Kevin Churchwell, a slender man in a sharp suit who serves as the CEO of Boston Children’s - a pediatric ICU physician by training who would later tell the Boston Globe that “panic is for wimps”, a statement full of bravado if I’ve ever heard one.
Three seemingly unrelated decisions happened shortly after the second Trump inauguration: cutting NIH research grants, limiting foreign visas, and settling scores with Harvard. Boston Children’s felt all of them. The hospital receives roughly $230M in NIH research funding annually - third-highest among all hospitals in the country. Immigration restrictions threatened the international researchers who run the most advanced pediatric studies in the world. And they’re literally right next door to Harvard Med School - a teaching hospital affiliation that was purely prestigious until it became a political liability. It was a flurry of blows, with the knockout punch still winding up.
The Medicaid cuts in the One Big Beautiful Bill Act (OBBBA) landed the biggest hit of all. For those who aren’t healthcare policy wonks: OBBBA cuts nearly a Trillion in Medicaid spending over the next decade. The major provisions (work requirements and redeterminations, among others) don’t take effect until December 2026, but pediatric hospitals are already losing sleep.
Nearly half of all children in America — about 37 million kids — are covered by Medicaid or CHIP. What Medicaid pays doesn’t cover what it actually costs to treat a child, so states negotiated supplemental payments to close the gap. Nearly two of every five Medicaid dollars children’s hospitals receive now flow through these supplements, and the OBBBA caps them. People assume the cuts won’t touch kids, but it’s hard to imagine a future where struggling hospitals keep unprofitable pediatric service lines open.
The past year was filled with questions from clients — hospital COOs, FQHC directors, a Medicaid managed care plan I was working with — all trying to decipher what the Medicaid cuts would actually do to their organizations. I’d been wrestling with this since October (wrote a version of this essay, was too chicken to post it), but eventually gathered the courage to call out the Medicaid doom loop in January. “Teach them well and let them lead the way” - my hot take: pediatric hospitals are the best model to predict how Medicaid will impact American healthcare.
Not Small Adult Hospitals
There’s probably not a more venerated building in the world than a children’s hospital - what could be more sacred than a place that heals the future of society? Which is odd because the economics of pediatric care are wildly underanalyzed across health policy - everyone models policy impacts of adult specialties. But if you want to model out healthcare policy at a small scale, it’s easier to study the ~250-ish pediatric hospitals rather than the 6000+ hospitals across the country. Children’s hospitals are a great microcosm: they’re geographically spread out, but people are willing to travel further for pediatric care.
Until I became a parent, I never thought about who runs the pediatric emergency room, or what happens when the nearest one closes. My son had a run of allergy episodes, literally on the night he turned one — swelling on his face, multiple ER visits in a couple of months — and the policy question isn’t abstract when it’s your baby.
Children are not small adults. A six-month-old metabolizes drugs differently than a six-year-old, who metabolizes differently than a sixteen-year-old… pediatric dosing requires weight-based calculations and specialized formulations. You can’t just cut an adult pill in half. Children’s hospitals operate as a completely separate network from adult healthcare, with their own economics, their own referral patterns, their own geography.
And their economics are uniquely exposed. Compared to about twenty percent of adults, the majority of children are covered by Medicaid. Children’s hospitals can’t chase commercial volume the way adult hospitals can; it’s not like other businesses where you can just sell more widgets to customers who can afford it. You’re not going to drum up elective hip replacements on eight-year-olds. And if a kid shows up in the ER, you’re legally required to treat them - regardless of what your CFO thinks of the payer mix.
Children’s hospitals aren’t even the first layer to feel it: the pediatricians and specialists out in the community, the small practices where families actually take their kids, are even more exposed and have none of the safety net a hospital does — no endowment, no philanthropy, no backup when Medicaid doesn’t cover the cost — and when those practices close, their patients end up at children’s hospital clinics.
There are also far fewer of them and parents like me are willing to drive as far as it takes to see a pediatric specialist, which means each institution’s reach extends wider and each closure displaces patients across more geography. Margins across children’s hospitals have already collapsed from double digits to barely one percent.
Children’s hospitals make up about five percent of the hospital market, but they’re a compressed version of every pressure facing American healthcare - the same dynamics, playing out faster and with nowhere to hide. What that looks like, up close, starts in Boston.
Where the World Comes for Answers
Boston Children’s motto is “where the world comes for answers“, which sounds like marketing until you learn that the hospital runs a Global Services department coordinating care for families from Gulf countries. Wealthy oil sheikhs bring families to Boston because there is nowhere else on earth that can treat their children - and BCH runs the largest pediatric research enterprise in the world, pioneering research in sickle cell anemia and cystic fibrosis.
But they’re dependent on the most vulnerable members of society - poor children.
Forty-six percent of BCH patients are covered by MassHealth (Massachusetts’ Medicaid program), and the hospital loses over $250M a year providing care for publicly insured kids. Sixty percent of their most medically complex patients — the ones with conditions so rare or severe that only BCH has the expertise — are on Medicaid. The hospital operates at a negative four percent operating margin — in an industry where breaking even is a good year — and stays afloat through investment returns and philanthropy.
Where the world comes for answers - and half the patients Medicaid-dependent.
Down the Pike
The oncoming storm doesn’t rain on BCH alone: other pediatric hospitals feel it even more deeply. In 2022, a struggling Tufts Medical Center closed the Floating Hospital for Children, because adults are more profitable - and redirected nearly two thousand kids a year to Boston Children’s. One closure in Boston, where alternatives exist.
Where I live in Worcester — forty-five minutes west — UMass Memorial Children’s posted an $87.5M operating loss in nine months, closed the state’s only teen substance use detox center, and shuttered psychiatric programs. I see their ads everywhere — YouTube, billboards, a campaign called “Relentless” — because when your pediatric families are drifting toward Boston, you spend money you don’t have trying to hold them. Specialist wait times are stretching to two months - parents in Worcester are calling Boston Children’s because they can get seen within a week.
My hometown of Springfield is nearly two hours west, and Baystate Health — the safety net for all of western Massachusetts — has slashed jobs losing a combined $300M since 2022 . The CEO, Peter Banko, projects the OBBBA will cost Baystate $146.7M annually, and he’s said publicly that “pediatric health care is among the valuable programs that don’t make money that would close in the community”. My high school buddy Keno has four kids - if Baystate can’t handle pediatric emergencies (and Banko basically telling us it can’t), Keno is driving his kids two hours east to Boston.
And even further past the state lines, the same issues bring it all back to Boston. Connecticut Children’s is closing its satellite unit in Waterbury - average daily census dropped to 1.3 patients, and you can’t staff a unit for a number that rounds to 1. In Maine, MaineGeneral closed its pediatric center after 67 years - 80% of its kids were on Medicaid. It’s not hard to imagine that parents in Connecticut and Maine are willing to travel even further into Boston.
BCH and Mass General for Children now handle 58.1% of pediatric discharges in the state — nearly six in ten kids who need a hospital bed — up from roughly half in 2011. Every closure that sends patients to BCH makes it more dependent on the Medicaid funding being cut.
It’s like when every side street goes under construction and the main highway gets congested - the highway wasn’t designed for this volume, and building new lanes takes a decade you don’t have.
One Big Beautiful Irony
Medicaid spending has been growing faster than almost anything else in the federal budget. Some states have gotten “creative” with supplemental payments in ways that are, in some cases, straight up gaming the federal match. So when it’s time to trim the federal budget, the logic seems straightforward: slow the growth, close the loopholes, reduce the government’s role. But Econ Policy 101 missed the part where cutting payments doesn’t reduce dependence - it concentrates it.
This is why I looked at pediatrics, it’s easier to model out here, but it applies in other spaces in healthcare too. Simply put, struggling hospitals can’t serve poor patients, the better hospital absorbs them, but then, it’s stuck with more poor patients. The flagship becomes more dependent on the extra funding that keeps it solvent - ironically the same payments capped by the OBBBA. Kids who lose coverage still show up at the ER, and the hospital absorbs more uncompensated care. The hospital’s own filings show it - BCH absorbed nearly seven thousand additional days treating Medicaid kids in just two years, meaning roughly half the beds in the hospital are now occupied by publicly-insured children, before the bill had even passed. A policy designed to shrink the government’s role in healthcare ends up concentrating it into fewer institutions that become too critical to let fail.
History rhymes with itself: the Balanced Budget Act of 1997 - or BBA, the older cousin of the OBBBA — cut Medicare spending to teaching hospitals and overshot the target by $88 Billion (!) — Congress had to pass emergency relief to undo the damage. The money came back, but the smaller programs that closed during the crisis didn’t - Congress funded the concentrated system, not the distributed one it replaced, and teaching hospitals ended up more dependent on federal payments than before the cuts started.
Think of it as cutting water to a garden. The deep-rooted plants survive by tapping reserves the shallow ones don’t have. The shallow ones die. But the survivor inherits everything the dead plants used to carry, and ends up needing more water than the whole garden did before the cuts. The bill meant to lower government-dependency, increases it.
State by State
It’s hard to imagine a life outside New England (is there such a thing?), but the dynamic plays out around every major pediatric flagship in the country - each at the center of a region where surrounding hospitals are shedding services and patients are concentrating inward.
I have consulting colleagues do real estate planning for Seattle Children’s, since it covers nearly a million square miles — Washington, Montana, Idaho, and cold-ass Alaska — and more than half its patients are on Medicaid. Alaska has no Level I pediatric trauma center - critically ill children transfer to Seattle by Learjet. These aren’t the same closures in Mass; they’re pediatric care deserts where the infrastructure never existed, and the cuts will only widen them. A pediatric cardiologist at Seattle Children’s, told a senator that without the hospital, “these babies could die, frankly, because they wouldn’t be able to get diagnosed.” Seattle’s Medicaid share of inpatient days jumped from 28% to 36% in just two years - one hospital absorbing the pediatric needs of five states, growing more government-funded with every patient it takes on, not less.
In Philadelphia, CHOP added 56 beds and $671M in revenue between 2022 and 2024 - expanding into the vacuum. Across town, St. Christopher’s Hospital for Children watched its commercial patients leave for CHOP and survives on a $76M local tax scheme — exactly the kind of supplemental payment the OBBBA caps. Just across the state line in Wilmington, Nemours Children’s — where BCH’s Dr. Churchwell was CEO before coming to Boston — is now under federal investigation and scrambling to invent an entirely new payment model to survive Medicaid instability. If any of them shutter services, the kiddos end up at CHOP - already at 91% occupancy, basically bursting at the seams (85% is considered at-capacity).
In every market, the flagship absorbs what the regionals shed. But that assumes there’s a flagship.
Where There Are No Deep Roots
And then you look at a place like Mississippi: where rural children already face double the mortality rate of urban children, where infant mortality runs 8.5 per thousand live births and for Black infants, 11.9 — the national average hovers around 5.5 — and the whole dynamic breaks, not because the mechanism is wrong, but because there’s nothing to concentrate into.
Greenwood Leflore Hospital sits in the heart of the Mississippi Delta — Leflore County, where more than half of children grow up below the poverty line. Before the pandemic, it was a 208-bed community hospital. By October 2022, it had closed its pediatric unit, its labor and delivery ward, and its ICU. By 2023, it had suspended use of 173 of its 208 beds, sold off neurosurgery and urology, and shuttered dialysis and rehab. What remains is an emergency room and some outpatient services. A shell.
The state’s only children’s hospital — Children’s of Mississippi, in Jackson — is two hours south and not nationally ranked in any pediatric specialty. Mississippi never expanded Medicaid; the OBBBA closes the door on ever doing so. A parent in Greenwood with a sick kid has three options: drive two hours and thirty-seven minutes to Jackson on a Medicaid salary with one car and no public transit, take the child to a rural ER that likely lacks pediatric equipment, or wait and see if it gets better. The data can count the first two options. It can’t count the third, but as a parent, I couldn’t fathom being stuck without the option.
What separates Boston from the Delta isn’t the policy, it’s what was already there when the cuts arrived.
Children’s Hospital Deserts
Two outcomes, determined by one variable: is there a deep-rooted institution in range?
If there is — BCH, CHOP, Seattle Children’s — the flagship absorbs what closes around it, each through a different route: in Boston, nearby closures funnel patients inward; in Seattle, the alternatives were never built, so one hospital covers five states by default; in Philadelphia, CHOP expands into the vacuum until there’s no capacity left to absorb more.
If there’s no deep-rooted institution — the Delta, rural Montana, the communities where the nearest children’s hospital is two hours away and not nationally ranked — care doesn’t concentrate. It vanishes. The first outcome is the irony — every closure meant to discipline spending just shifts the weight to fewer institutions that become harder to walk away from. The second outcome isn’t ironic at all, just a straight line from funding cuts to gone.
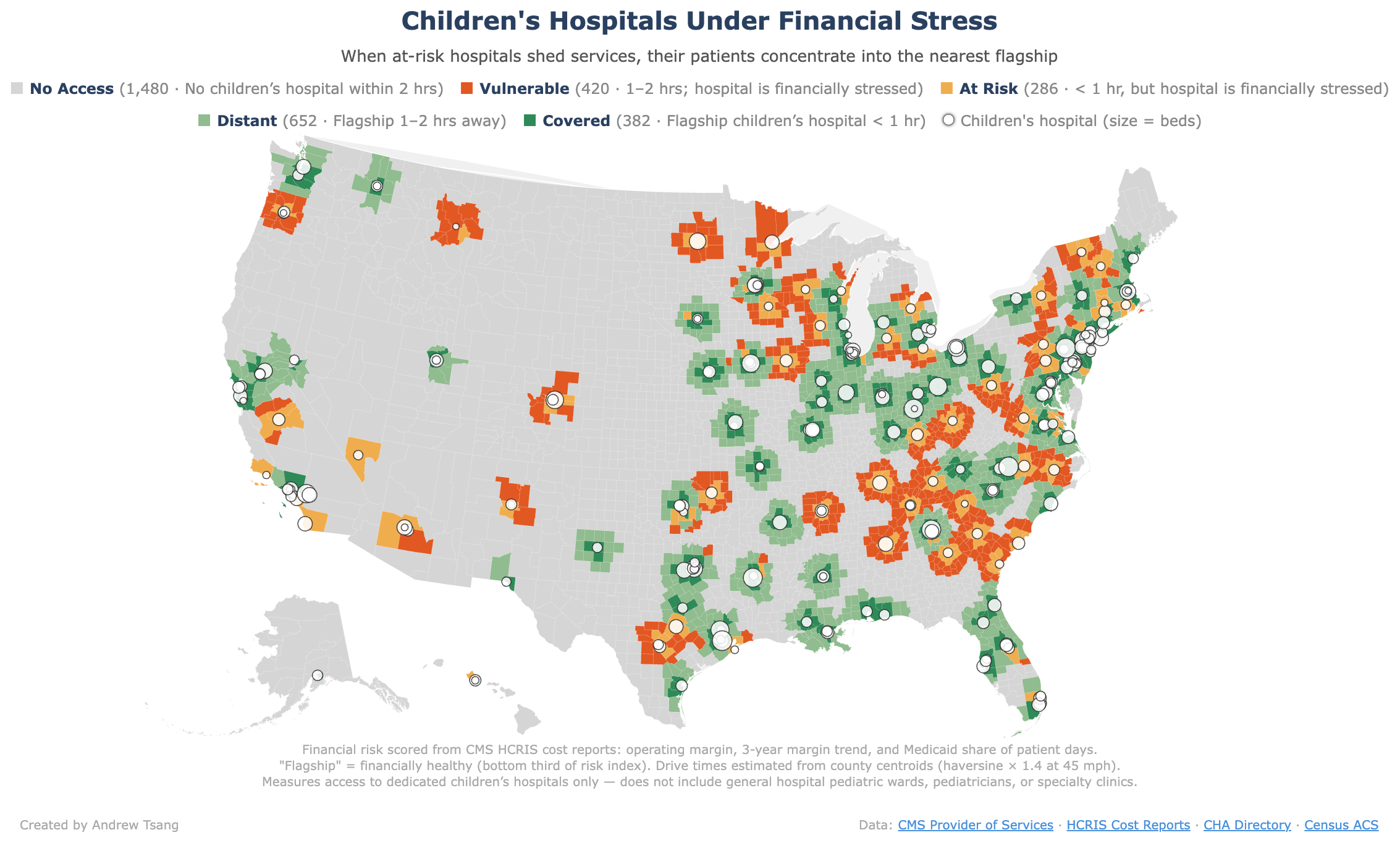
You could draw circles around the twenty or thirty elite children’s hospitals in the country and say with reasonable confidence what happens inside each radius versus outside all of them. Inside the circles, the flagship gets bigger and more government-dependent. Outside the circles, care thins out until it’s gone. Three states — Wyoming, Idaho, Montana — have no freestanding children’s hospital at all. Trace a two-hour drive radius and nearly half of all counties fall outside every circle - about 13 million children with no children’s hospital within a reasonable drive, which is manageable if your kid has a scheduled appointment - but not if your kid suddenly starts wheezing at 2AM.
And a lot of those circles are drawn around hospitals that are already in financial trouble - institutions running at negative margins, shedding services, closer to the next Tufts closure than the next CHOP expansion. Roughly thirty-two million children, about 43% of all kids in the country, live in a county that is either already a pediatric care desert or one hospital closure from becoming one.
Each closure erases a circle from the map and pushes those patients toward whatever flagship is left, which absorbs them, runs hotter, and becomes more dependent on the public funding that the OBBBA caps. But the flagship that inherits the patients also inherits the vulnerability - a hospital that was 46% Medicaid-dependent at the start of the cycle is 55% dependent after absorbing the closures around it, which means the next round of cuts hits it harder, which means the circle everyone assumed was permanent starts to look fragile too.
The Grown-Up Version
Pediatric hospitals model the dynamic, but they don’t own it. Before someone accuses me of using sympathetic children as a cudgel to make my point - fine, let’s talk about pregnant women instead. Take rural obstetrics: Medicaid covers about 40% of all U.S. births nationally, rising to 50% in rural areas and around 60% in states like Louisiana - the same lopsided dependence on Medicaid. You can’t upsell a C-section, you can’t market your way into more commercially insured pregnancies (maybe a campaign for increasing procreation?), and your patient volume is determined by whoever lives in the area and decides to have kids, which doesn’t exactly show up on a CFO’s strategic plan. And the expertise is spread thin in exactly the same way pediatrics is.
One hundred and seventeen rural hospitals have stopped delivering babies since 2020, and 59% of rural hospitals no longer offer obstetric services. The March of Dimes coined the term “maternity care deserts” (inspiration for my Children’s Hospital Deserts), which illustrates that a thousand counties — a third of the country — are classified as maternity care deserts, with no birthing facility and no obstetrician.
The same two outcomes are visible. In Maine, twelve birthing centers have closed in the past decade — four in 2025 alone — and virtually all obstetric training and care concentrates toward Portland, the state’s single remaining OB residency program pulling the gravity of the whole system toward one city, and becoming more Medicaid-dependent with every closure it absorbs. In the Delta, Greenwood Leflore lost its maternity ward along with everything else - mothers now drive a hundred miles for prenatal care, and the state declared a public health emergency over infant mortality in 2024, the highest rate in a decade.
Obstetrics is actually more vulnerable: children’s hospitals are freestanding institutions with their own endowments, their own research enterprises, their own philanthropic bases. Maternity wards are service lines inside general hospitals — in the language of hospital finance, delivering babies is a product line — and when a hospital needs to cut a money-losing department, labor and delivery is often the first to go. There’s no freestanding equivalent of Boston Children’s for obstetrics — no institution with the depth of roots to be the last one standing. Which means in many parts of the country, there’s no institution to absorb what closes, and the maternity care just disappears.
The same conditions — most patients on Medicaid, specialists few and far between, no way to make it up on privately insured patients — show up in burn care, where 130 centers serve 330 million people and eight states have no burn center at all, and in psychiatric care, where 169 million Americans live in a mental health shortage area and nearly 59% of counties have never had an inpatient psychiatric bed. Each follows the same fork: where a flagship exists, it absorbs what closes around it and grows more government-dependent; where there’s no flagship, care disappears. Any specialty that serves patients who can’t choose their provider or their payer is running the same finances - and there are more of them than anyone is counting.
Too Essential to Fail
The worst of it hasn’t arrived yet. Work requirements take effect in December 2026, the heaviest Medicaid cuts land through 2027 and 2028, and the rest of the cuts phase in through 2032.
The policy was built to shrink the government’s role in healthcare - slow the spending, close the loopholes, let the market absorb what government retreats from. What it’s producing, in every system where you can trace the effects, is fewer institutions doing more of the work, more dependent on public funding than the landscape they replaced, too essential to the communities they serve for any administration to let them fail. The opposite of the stated intent, arrived at by the most direct route possible.
Every few years the country will have some version of this argument — how much to spend on Medicaid, where to cap it, who qualifies — and almost every time it will be about the dollars, not the infrastructure underneath them, not the question of what happens to institutions you can’t rebuild once you’ve let them close.
Whether that’s better or worse probably depends on whether you’re a sick kid in Vermont who now has to travel to Boston, or a sick kid who gets access to world-class care they wouldn’t have gotten at their regional hospital. Or whether you’re a kid in the Mississippi Delta who doesn’t get to make the trip at all.
Separate from your point about the OBBB weakening hospital finances generally, and the generally-recognized point that about 10 million people will eventually lose coverage from it, I have a third observation.
There will be numerous administrative and paperwork verification burdens, such as, but not limited to, work verification and more frequent verifications of various other program requirements.
These complex verifications need to be done by 51 separate state +D.C. Medicaid agencies, a federal exchange, and 22 state exchanges. (ACA exchanges get involved because eligibility for any Medicaid, including expanded Medicaid, makes one ineligible for subsidized on-exchange coverage under ACA rules.)
I count 21 million people getting expanded Medicaid alone, and about 22 million entities people getting on-exchange ACA coverage.
Now, I have experience with a pair of those state agencies in my own state, over the 2014 to 2022 period when I used the ACA for my own coverage. (I have aged into Medicare-for-me!)
God bless them, some of those state agencies are under-resourced, and not that technically adept. (I was in primal fear myself of having no health insurance, despite always being eligible, and never making any mistakes in applying, at least five times in those 9 ACA years!)
I can't imagine that we won't have a big mess here. People who are supposed to have coverage under BBB not having it for long periods of time. Frustration, and time wasted, by people trying to document their eligibility.
More precisely, about 51 unique big messes, that each have their own custom-by-state flavor, starting a few months before the main OBBB Medicaid stuff goes into effect Jan 1, 2027.
It will be interesting to see exactly how it goes!
The kicker? About 4-5 million kids under 18 are uninsured - and about 1/3 of them are eligible for Medicaid but aren't enrolled. Imagine the fiscal pressure if we added ~1.5 million kids ...
"It boggles my mind that the same people who cry 'foul' about rationing an instant later argue to reduce health care benefits for the needy, to defund crucial programs of care and prevention, and to shift thousands of dollars of annual costs to people - elders, the poor, the disabled - who are least able to bear them." Don Berwick